
The White House is asking Congress to sharply roll back federal spending on HIV prevention, a reversal from President Trump’s first term, when he championed investment to end the epidemic in America within a decade.
President Trump, in his first term, urged Congress to spend more in the nation’s decades-long fight against HIV and AIDS. “We have made incredible strides — incredible,” the president said to applause during his State of the Union address six years ago. “Together we will defeat AIDS in America and beyond.”
In that speech, he set out one of the most ambitious health policy goals of his administration: End the HIV epidemic in the U.S. in 10 years.
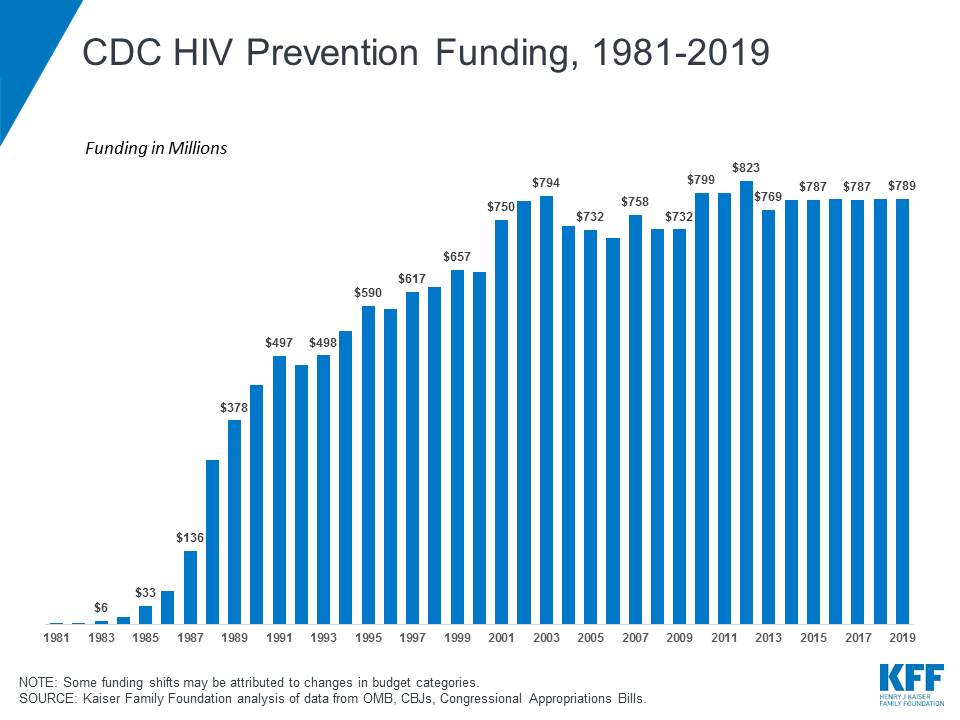
That initiative may now stop five years early. President Trump is back in office with new priorities. The White House budget proposal would roll back next year’s federal HIV prevention funding to levels not seen since around 1987. Much of that funding typically flows to local public health agencies and nonprofits to test for infections, monitor for outbreaks and promote prevention.
No money is flowing at the moment. The administration this month froze at least $460 million for grants to local public health and nonprofits that were scheduled to start June 1.
The president’s reversal is paralyzing HIV prevention work nationwide, advocates, researchers and public health experts told Tradeoffs.
“Does this administration simply want HIV prevention activities to go away, and by extension, want additional HIV infections throughout America?” said Jeremiah Johnson, executive director of the advocacy group PrEP4All. “Because there’s simply no explanation of what else this could possibly achieve.”
How the U.S. funds HIV prevention (for now)
The Centers for Disease Control and Prevention is the federal agency that oversees HIV prevention. It has been spending about $1 billion a year on those activities, including roughly $220 million for Trump’s first-term initiative.
The White House is now asking Congress to strip nearly $800 million from that spending. City and state budgets would be squeezed by the loss of those funds, much of which is sent to cities and states to pay for epidemiologists to track infections, for free HIV tests and self-testing kits, and for various types of prevention outreach.

Andrew Nixon, spokesman for the Department of Health and Human Services, said HIV prevention continues to be a high priority for the administration, and critical activities will continue under the new Administration for Healthy America.
The U.S. spends far more on HIV and AIDS treatment — largely through Medicare and Medicaid — than on HIV prevention, even before Trump’s proposed cuts. Public health and infectious disease experts say the nation could save by investing more to stop infections, which costs about $500,000 over a lifetime to treat.
Trump’s proposal would cut HIV prevention under the CDC by 75%, reducing spending to a level not seen since the U.S. launched its first AIDS public service announcement in the mid 1980s.
For anyone old enough to remember the early years of the HIV epidemic, prevention has come a long way. As it became clear the virus could spread by sex and contaminated needles, public health agencies recommended condoms and safe needle exchanges. It was, understandably, an imperfect defense.
“I went through this myself. You hear your whole adolescence and into young adulthood, the best way to not get HIV is to not have sex,” said John Brooks, an epidemiologist and doctor who has spent his career fighting the virus. “Nobody’s a saint.”
It was, however, the best defense available for about a quarter of a century. That changed radically in 2012, when regulators approved a daily pill that can block an HIV infection. The treatment is known as PrEP, for pre-exposure prophylaxis.
Brooks, who retired last fall as medical director of the CDC’s HIV prevention division, described PrEP’s discovery with something like awe: “It was astonishing, the potency of this simple intervention.”
Trump’s Big Swing to End the HIV Epidemic
PrEP is critical to Trump’s initiative to end the epidemic by 2030.
By 2019, as the initiative launched, PrEP had been on the market for years, but had failed to take off. Getting more people on this medication is a key strategy to halting the epidemic.
It’s also one of the biggest challenges for reaching the president’s target. The costs involved in taking the medication, including occasional lab work, and the stigma that persists around HIV keep many from talking to doctors about a prescription, say advocates. Some doctors and pharmacies don’t offer the drug, creating what are known as PrEP deserts.

Through last year, Congress has poured $2.3 billion into the president’ initiative, including extra funding to HIV hotspots for PrEP advertising, outreach and screening.
That money is critical if the nation wants to bring the virus under control, said Brett Giroir, one of the first-term Trump health officials who helped get the effort started. But the administration’s backing for the initiative’s ambitious target was crucial, too, he said. “Money without leadership is nothing. You’re just throwing it away.”
PrEP use has increased nationwide, to roughly 30% of those who would benefit, up from 22% before the initiative got underway. But that’s still short of the 50% target to meet the initiative’s 2030 deadline for halting the epidemic. One analysis published this year by CDC researchers found no extra gains in PrEP use in places targeted by the initiative. But the authors cautioned that the pandemic disrupted the initiative’s early work, so impact of programs may not be visible yet.
Threats of Funding Cuts Have Already Stopped Some HIV Prevention Efforts
In Tulsa, Okla., the nonprofit organization called Health Outreach Prevention Education, or HOPE, has made progress in boosting PrEP use, but its successes take time.
HOPE staffs clinics and mobile vans that bring HIV tests and promote PrEP across the city and nearby rural areas — partially funded by the president’s initiative and other HIV prevention grants from the CDC.
Brad Sullivan is one of HOPE’s success stories. He had seen HOPE’s outreach staff around Tulsa over the years, he said, and knew he was overdue for HIV testing and PrEP. But it took his friends having a scare with a sexually transmitted infection to get him to finally talk to a HOPE staffer and start on PrEP.
Had HOPE’s program not existed he might not have gotten tested, Sullivan told Tradeoffs. He would feel too vulnerable to have a conversation about HIV at his primary care clinic. Sullivan is gay and 53. He grew up in rural Oklahoma and attended Christian college before he came out.
“You live with that fear of rejection from loved ones,” he said, “from friends, from people you may just be a casual acquaintance with.”
He didn’t feel that fear with HOPE. “You’re going in there and you’re talking with people that get it,” Sullivan said.
Hana Fields, HOPE’s outreach manager, said she hears ‘no’ often from people she talks with about PrEP, as she visits spots around the city.
Some tell her they are uninsured and fear they can’t afford the treatment. Others have never heard of it. Many say they can’t travel across town to HOPE’s clinic for the exam and tests they’d need to start the medication.
Despite repeated “no’s,” Fields and her team keep showing up time after time, to get the word out on PrEP and to build trust. Sometimes, eventually, it works, she said. “If you are there enough in a person’s life, you will catch them on the day that they’re ready to start taking action.”





Sterile syringe kits sit inside of a vending machine at HOPE’s clinic in Tulsa. Credit: Nick Oxford for Tradeoffs


{kind=link}
Much of HOPE’s federal funding is now up in the air. The Trump administration froze the HIV prevention grants from the CDC that were scheduled to start this month.
The HOPE program was counting on that money, and now Taryn Norman, HOPE’s executive director, finds herself poring over the nonprofit’s finances, trying to figure out how long their cash will last.
The worst case scenario, Norman said, would force HOPE to stop some of its work and lay off staff.
Oklahoma last week advised HOPE to limit HIV prevention spending to necessities, Norman said, until the federal government makes it clear when it will release CDC grant funding. Public health agencies elsewhere have taken more aggressive steps. The Arizona Department of Health Services told organizations it funds with CDC grants to stop their HIV prevention work, such as helping people get PrEP prescriptions.
If CDC funding eventually comes through, the state will try to pick up where it left off, the agency said in an email to Tradeoffs, adding “The longer the delay in funding lasts, the harder it will be for organizations to bring services back.” Los Angeles County and North Carolina have also halted funding for local HIV prevention efforts.
Federal Turmoil Could Squander Investment, Reverse Gains
Threats of funding cuts are the latest in White House actions that, combined, would gut the nation’s defenses against HIV, say public health leaders and HIV prevention advocates.
Mass layoffs at the Health and Human Services Department included HIV prevention teams at the CDC — teams needed to do the analysis of HIV infections and PrEP use nationwide. Much of that work stopped with the layoffs, though the agency said this month it would rehire some people who do work on HIV and other sexually transmitted diseases.
Trump’s HIV initiative also poured money into studies of how best to increase PrEP use among high-risk groups, including transgender women, Black women and gay and bisexual men.
But several of those studies abruptly lost funding when the President issued executive orders to eliminate equity initiatives and policies. For studies of LGBTQ+ health alone, the administration terminated about $800 million in research, according to a recent lawsuit.
Congressional Republicans, meanwhile, are pushing ahead with plans for new Medicaid enrollment rules that would remove millions from that safety-net health insurance program. Medicaid coverage is one factor associated with higher use of PrEP, studies find.
“Any hope of ever ending the HIV epidemic is very much tied to a functioning Medicaid program,” said Amy Killelea, an assistant research professor at Georgetown University and public health law expert.
The upheaval also threatens to squander potential progress from a longer-lasting version of PrEP approved by the Food and Drug Administration this week.
The new drug, lenacapavir, is highly effective at stopping infection, as are existing drugs on the market. But other versions of PrEP must be taken daily or, at best, every two months, with schedules that have been hard for some people to maintain. A single dose of Lenacapavir protects against HIV infection for six months. Researchers’ estimates suggest having this sort of less-demanding option available can further reduce infections.
“It really does change things considerably by virtue of its long-acting effect,” said Jim Kublin, a principal scientist at the Fred Hutchinson Cancer Center who is working to develop an HIV vaccine. But the powerful new drug option will need formidable outreach to reach enough people to make a difference, he said, or “its eventual impact will be far inferior to the initial enthusiasm we may have had.”
Episode Transcript and Resources
Episode Transcript
President Trump: Scientific breakthroughs have brought a once-distant dream within reach.
Dan Gorenstein: That is President Trump. This is the year before COVID hit. 2019.
The president is speaking before Congress.
It’s his State of the Union address, the big, showy speech when U.S. presidents lay out their policy priorities.
DT: My budget will ask Democrats and Republicans to make the needed commitment to eliminate the HIV epidemic in the United States within 10 years.
DG: It’s a policy goal that’s about as ambitious as you can get for the nation’s decades-long response to HIV, the virus that causes AIDS.
DT: We have made incredible strides. Incredible. (Applause) Together we will defeat AIDS in America and beyond. (Applause)
DG: Trump got what he wanted.
Congress started to pour more money into the fight. Even after Trump left office … the U.S. continued to invest hundreds of millions of dollars year after year into research, safety net clinics and local public health efforts aimed at ending the U.S. HIV epidemic.
Now,
News clip: the White House unveiled a budget proposal today that would cut billions from non-defense programs across the government.
DG: …President Trump is back in the White House … with new priorities.
DG: this vision is at odds with the aggressive goal he laid out six years ago.
Today, to understand what Trump’s return to office means for maybe the boldest health policy goal of his first term … we look at a key to his plan to end the HIV epidemic … Getting more people on drugs that stop infections.
From the studio at the Leonard Davis Institute at the University of Pennsylvania, I’m Dan Gorenstein. This is Tradeoffs.
DG: One recent morning in Tulsa, Oklahoma, Hana Fields climbed into a white van with her tackle box of HIV test kits, ready to head out for work.
Sound from parking lot
DG: Hana works for a nonprofit called HOPE.
A few days a week, HOPE sends vans across the city and into nearby rural counties to offer HIV tests.
Sound from parking lot
DG: The vans turn up at nightclubs, community centers or … on request.
HOPE has a profile on dating apps, so people can reach out that way too.
Hana Fields: We’ll go to people’s houses, we’ll meet people at parks. People will sneak out of their jobs on their 15 minute breaks. Testing is so important, Um, and so heavily stigmatized that we will try to get a hold of communities that need testing, kind of by any means necessary.
Sound of driving
DG: Hana – who is HOPE’s outreach manager – has an easygoing manner.
She knows when she talks about how to protect yourself from HIV … that conversation can get super personal, super fast.
She’s direct as she talks about sex and drugs, two primary ways the virus is transmitted.
HF: I have been stigmatized, treated like shit in medical systems. I have waited a long time for care that I needed. So now I do my best to be warm to anyone that I come in contact with, because I think it’s right.
DG: DG: Hana and her co-worker head to a local church parking lot.
Sound from driving HF: If somebody wants a Hep C test, we could just use the sure check for HIV since they’ll be there for 20 minutes anyway…
DG: The two park the van strategically … so it’s easy to be seen.
People who are homeless come here to use mobile showers and wash their clothes.
It’s sunny, muggy and very windy.
Sound from set up HF: Do you by any chance have any tape anywhere? I didn’t think about the wind
DG: The pair set up a folding table with free condoms and flyers.
Sound from set up HF: I found the tape. (Whoo!)
DG: Testing for HIV is important for a few reasons.
One … the virus can go undetected for years before symptoms emerge.
Two … testing also is this kinda perfect opening to talk to people about the medication … called PrEP.
If taken regularly, PrEP can prevent an HIV infection.
HF: It is really nice to be able to, like, ease into a conversation about Prep, especially because we live in Oklahoma, where a lot of people don’t even know what it is, or don’t know that it would be an option that would potentially work for them.
DG: Getting this drug to as many high-risk people as possible is crucial to stopping the epidemic.
Hana tested three people for HIV that day in the church parking lot.
They all tested negative. With each, she walked through how to get a prescription for PrEP. No one took her up on it.
Most people tell Hana ‘no.’ For all kinds of reasons.
HF: Then there’s, you know, like rides to the clinic. don’t feel like they could get on health insurance. people really don’t like blood work. So just some small barriers that become, like, huge.
DG: HOPE sends these vans to the same places … again and again, says Hana, to get the word out on PrEP, of course … big picture, they’re just trying to build trust with people who have a hard time trusting anybody.
HF: If you are there enough in a person’s life, you will catch them on the day that they’re ready to start taking action.
DG: But as much as Hana may want to … she may not be back.
Each year the CDC spends some $1 billion on HIV prevention … but the president has proposed an $800 million cut to those funds.
Much of that money goes to places just like HOPE for work to stop the spread of HIV among high-risk people … with big barriers to care.
Jeremiah Johnson: Does this administration simply want HIV prevention activities to go away, and by extension, want additional HIV infections throughout America?
DG: That’s Jeremiah Johnson, executive director of the advocacy group PrEP4All.
He says the proposed change would gut the work.
JJ: Because there’s simply no explanation of what else this could possibly achieve in terms of the HIV epidemic.
DG: Jeremiah’s group promotes broad use of PrEP … which … has been a key pillar in Trump’s bold initiative to end the HIV epidemic.
The existence of PrEP, in fact, is what helped make that bold effort possible in the first place.
The drugs were introduced in 2012. They were considered game-changing — a strong new defense against the spread of HIV where existing alternatives … condoms, say, or abstaining from sex … might fail.
News clip: Scientists call it PrEP. That stands for pre-exposure prophylaxis.
News clip: When taken every day, PrEP can reduce the risk of getting HIV from sex by more than 90%.
News clip: I think this is a huge milestone. I think we are in an era now, for the first time, when we can foresee the end of the AIDS epidemic.
DG: Despite all the hope …PrEP failed to take off
There are many reasons why, including persistent stigma, lack of insurance coverage and the cost of prescriptions.
Brett Giroir got it. He knew all the reasons why so few people used PrEP.
But Brett really believed the U.S. could end the HIV epidemic … if we went all in on leveraging PrEP.
Brett was the assistant secretary for health in Trump’s first term. He was one of the people to come up with the initiative and pitch the idea to the president.
BG: We had the technology to prevent, with Prep. If you effectively treat, you can’t transmit by sex. Period. Zero. You know, we didn’t have to, you know, build the Apollo program. It’s just a matter of will. It’s not a matter of miracles have to happen. It’s a matter of will.
DG: Once Trump endorsed the initiative in 2019, Brett and health officials across the administration got to work.
They set a target: Get 50% of people who would benefit from PrEP using it by 2025.
But how to do it?
They poured money into community clinics to make PrEP more available … and new grants funded studies on how to get more people on PrEP.
Brett says they also went hyper-local with outreach. They wanted to do more than put up a billboard or buy a tv ad.
BG: I went down to Miami … we had a Catholic nun helping us, you know, promote PrEP. You got to have the last mile, right? So this was sort of public health 101.
DG: The first grants sought to curb infections where the data showed new HIV diagnoses were most prevalent. Black and Hispanic gay men in the south. Transgender women. Some rural areas. People who use injection drugs.
Hundreds of millions of dollars flooded into HIV hotspots. 57 different places.
BG: You pick jurisdictions that are the highest need and the hardest nuts to crack. And that’s what we did.
DG: Oklahoma was one of those spots.
HOPE, in Tulsa, gets some of that money. Those vans to test for HIV and promote PrEP? Paid for, in part, by Trump’s initiative.
DG: The dividend from this investment is the case of Brad Sullivan.
Brad, now 53 years old, had put off getting tested for HIV for years.
Then several friends had an STI scare – a sexually transmitted infection scare.
Brad Sullivan: You may not know your status…and a lot of times there’s a lot of people that are okay with that. until, you know, like, for me, it was…I need to do this … this is … this is dumb. I need to… … take control of my own health There’s no reason I shouldn’t. It’s 2025.
DG: Brad knew just what to do.
He’d seen HOPE’s outreach staff turn up at Tulsa clubs and an LGBT community center where he taught.
BS: You’re going in there and you’re talking with people that get it
DG: Brad Sullivan perfectly fits the profile of who the Trump initiative had hoped to reach … someone who is at high risk … but is not on PrEP.
I asked him would he have sought out PrEP if HOPE didn’t exist.
BS: That would be a tough call there…It would lean probably closer to the not doing it. To be quite honest.
DG: He said he would feel too vulnerable anywhere else to have a conversation about HIV.
BS: You grow up and you live with that fear of rejection from loved ones, from friends, from people you may just be a casual acquaintance with.
DG: That fear is hard to shake, he says, growing up when and where he did … a small Oklahoma town. Brad came out after college.
BS: My name was going through the grapevine quick when…certain people in certain circles found out I was gay.
So now you’re looking at a whole group of people that you spent years with, and some may talk to you, some may not.
DG: That fear is amplified when his health is concerned. He knows his doctor is concerned for his health … yet when he thinks about going to his doctor …
BS: They may choose not to be a provider for you anymore. Now is everyone within that office, you know, talking. I mean,, a little paranoia can hit, and feeling judged again, you know, not me as a person, but for who I’m attracted to.
DG: The threat of discrimination … the hurt of rejection … those reasons help explain why HIV outbreaks continue to flare up in these hard-to-reach pockets in our country.
The best way policymakers have learned to combat those kinds of concerns is by funding outreach work … so when someone a lot like Brad, for whatever reason, happens to be ready to start PrEP … an organization like HOPE is ready for him.
DG: As of today, the administration has withheld at least $460 million for state and local HIV prevention grants that had been scheduled to start June 1. And that is putting HOPE funding for its vans up in the air.
When we come back, why advocates say Trump’s second-term priorities could pose an existential threat to the fight against HIV in America.
MIDROLL
DG: Welcome back.
HIV and AIDS experts say President Trump’s agenda to sharply cut federal spending is paralyzing work to end the HIV epidemic in America … a signature policy of Trump’s first term.
To understand what this looks like on the ground, we’re examining what his second-term policies mean for getting powerful HIV prevention drugs called PrEP out to more people.
In the first half of the show we looked at how the President’s moves have harmed outreach.
Tradeoffs producer Melanie Evans joins us to talk about what’s happening beyond that.
Hey Melanie.
Melanie Evans: Hi Dan.
DG: So we know that today – about 30% of people who could benefit from PrEP are taking it – that’s progress – back in 2019 it was just 22%.
But that is still a far cry where we need it to be if we’re going to stop the HIV epidemic.
ME: That’s right, Dan. Public health officials set a target of 50% by … this year.
So we’re a little bit behind where the first Trump administration wanted us to be.
To move that number … Public health officials say we need two things: Good data, to direct outreach where it needs to go, and research, to identify the most effective outreach strategies.
DG: OK. But all that requires people and funding … and this year the Trump administration is cutting both.
ME: Exactly. Let’s start with how that’s affecting data to track the virus’s spread.
The CDC is the federal agency responsible for monitoring the HIV epidemic.
DG: Right. The CDC collects data on where and how many new HIV infections are happening.
ME: Yes, and the CDC tracks data on the use of PrEP, to understand where outreach strategies are holding the line on infections.
I should say the CDC did track data on PrEP use. Mass layoffs in the last couple of months included teams that were focused on HIV prevention.
DG: This was part of the sweeping changes in HHS under Robert F. Kennedy Jr., right? Last month he told Congress his reshuffling would put more focus on chronic disease and do more with less.
ME: At least for now, Dan, HIV prevention offices that lost staff are doing less with less.
The CDC said last month it’s unable to update its data on PrEP use because of the layoffs. That’s a huge blindspot.
Patrick Sullivan: If public health were a business, this would be our business intelligence, this would be our, our data in which markets we’re doing well, in which markets we need to invest more.
ME: That’s Patrick Sullivan. He is the principal scientist behind an online dashboard that maps the virus and response efforts at Emory University. The dashboard relies on this CDC data.
Patrick’s been using it to pinpoint where there are gaps in PrEP use among people who could really benefit.
DG: That makes sense. If public health experts can identify and understand these gaps in who’s using PrEP and who’s not they will be better able to address the disparities.
ME: Yes…and the research shows … transgender women, Black and Hispanic gay men in the South and other groups, are at higher risk for HIV.
Patrick is worried that this data, which people have relied on for years, could be compromised or lost.
PS: It is going to be like halfway in a trip across the country and your GPS goes out and you have no map. Um, and there are no road signs. And it’s like,, maybe, uh, you can navigate by the sun and the moon.
ME: The CDC says it is quote “evaluating plans and capacity to resume this work.” and has rehired some HIV staff as of mid-June.
DG: Ok, Melanie. So, that’s how the mass layoffs at the CDC have undermined HIV and PrEP tracking.
You also said the White House agenda has hit other HIV research.
ME: It has. Trump’s HIV initiative poured money into studies of how best to increase PrEP use among those high risk groups.
Several of those studies abruptly lost funding this year when the President issued executive orders to eliminate equity initiatives.
DG: Right, he canceled a lot of health research, which we discussed on an episode earlier this year. For studies of LGBTQ+ health alone, the administration terminated about $800 million in research.
ME: Right … a lot of the studies have tried to figure out how to get the message …. that PrEP can save lives … out to people who were reluctant to talk to their doctor.
For example, one grant tested apps for transgender women.
Another looked at whether cognitive behavioral therapy could help Hispanic gay and bisexual men.
DG: I mean, this is the kind of work, I gotta imagine, that’s key to ending the HIV epidemic.
ME: That’s why the initiative invested in the research, in the first place, Dan.
I will say there’s a study from the CDC that looks at the results of this investment, so far.
Researchers found gains in PrEP use around the country, but no extra boost where Trump’s initiative targeted funds. The authors said the pandemic may have played a role.
I asked the administration about workforce and funding cuts.
Health and Human Services told me that HIV and AIDS programs are a high priority, and that critical work will continue.
DG: Melanie, all this is happening while we could see PrEP become unaffordable for some folks.
The Supreme Court will soon decide if most insurers must keep covering PrEP at no cost to patients. The drug will become much more expensive…if the court rules that insurance companies can start asking for a copay.
And, of course, you’ve got the Republican budget bill working its way through Congress which could result in millions losing coverage.
ME: Here’s the thing, Dan, the timing of all this upheaval overlaps with the expected release of a new, longer-lasting PrEP, called Lenacapavir. The FDA is expected to approve it soon.
DG: Right. I’ve heard about it. One dose of the drug lasts six months. Drugs on the market now must be taken daily or every two months.
ME: Yes, HIV experts I talked to are excited about how this new drug could make it easier to eradicate HIV and AIDS.
Of course, a new drug will be expensive, but a more convenient drug could mean more consistent use … and more people who stay protected.
But cuts to PrEP outreach staff and funding would make it harder to get the drug to high risk folks.
DG: Kinda squandering this innovation?
ME: That’s what the public health experts tell me.
And, Dan, one more thing. Lenacapavir is also interesting, because it’s an example of where the nation’s long-term investment in basic science research has paid off. This, too, is an area where the Trump administration’s new priorities call for deep cuts.
Wes Sundquist: I’m Wes Sundquist and I’m a chair of the Department of biochemistry at the Spencer Fox Eccles School of Medicine at the University of Utah.
ME: Some of the scientific advances that made Lenacapavir possible started out in Wes’s laboratory.
DG: I know how much you like science, Melanie. What did you learn from Wes about this?
ME: Indeed I do, Dan. Early in his career, Wes set out to understand one of the mysteries of HIV …
…a quirk in the shape of the virus.
His lab was asking very basic, science-y questions at a time when most other researchers were studying promising targets to attack HIV.
It turns out, the discoveries in Wes’ lab helped set the stage for the development of Lenacapavir by the drug company Gilead.
WS: When people study fundamental things, they make discoveries. And those discoveries, inevitably, as a field, lead to advances in medicine and often in very unexpected ways.
ME: Figuring that out took Wes and his team about 15 years. The whole time, he relied on grants from the National Institutes of Health to pay his salary and hire researchers.
WS: If we hadn’t had sort of reliable, steady funding, we just couldn’t have done the work.
ME: As I reported this episode, I just kept hearing about the extraordinary investment the U.S. has made to combat HIV and AIDs. Wes’s lab. Patrick’s research. Hope’s outreach.
What doctors and public health workers told me is the administration’s sudden and sharp pullback in federal funding could thwart that investment.
And it’s hard for some folks to wrap their heads around this kind of retreat
John Brooks: What is happening right now is something that I don’t think anybody ever imagined would actually happen.
ME: John Brooks has spent his career combating HIV and AIDS.
He retired a few months ago from his job as chief medical officer for the Division of HIV prevention at the CDC.
He spent more than two decades in the division. He remembers the early days of the epidemic.
JB: I’m gay. And, you know, you start to hear about this gay plague, this gay disease. It was terrifying. Terrifying. It wasn’t just terrifying for gay people. It was terrifying for all Americans because none of us knew. How was it transmitted? How could I get it? My God, how many people could I have exposed? How many people might have exposed me? It was terrifying.
ME: John said he can recall breakthroughs that began to tilt the fight against the virus in our favor … including PrEP.
JB: Look, I’ll be honest. I went through this myself. You hear the best way to not get HIV is to not have sex. And if you’re going to have sex, you have to use a condom. You need to reduce your number of partners. I mean, this is really a hard message to operationalize because each of us, as I sometimes like to say, have two brains.
ME: PrEP, says John, represented a very effective tool – one that could potentially cut the number of new HIV infections by about 48,000 over five years,
JB: It was astonishing the potency of this simple intervention, which used a medication that had very few side effects.
ME: Preventing an infection can, literally, be life changing.
It also avoids the cost of treating HIV over a lifetime … some $500,000.
John says he fears progress will dead end at a moment when the U.S. is … really, really close to ending the HIV epidemic.
But now, Dan, outreach funding has been cut … disease tracking halted … funds for research have disappeared.
The cumulative effect of President Trump’s actions are strangling this effort … so much so … that we could start to see HIV rates reverse … and start to climb.
DG: Melanie Evans, thanks for your reporting on this.
ME: I will, Dan.
Episode Resources
Additional Reporting on HIV prevention and PrEP
- HIV protection with just two shots a year: FDA approves Gilead drug (Jason Mast and Ed Silverman, STAT, 06/18/2025)
- An HIV Vaccine in the Era of Twice-Yearly Lenacapavir for PrEP — Essential or Irrelevant? (Lauren P. Jatt, Nyaradzo M. Mgodi, Susan P. Buchbinder, Glenda E. Gray and James G. Kublin, New England Journal of Medicine, 04/19/2025)
- Ending the HIV Epidemic (EHE) Funding Tracker (Lindsey Dawson, Tenzin Dhondup, and Jennifer Kates KFF 04/08/2025)
- What we’ve learned from federal efforts to fight HIV/AIDS (Soleil Shah, Tradeoffs, 05/02/2023)
- Why Is No One On the First Treatment To Prevent H.I.V.? (Christopher Glazek, The New Yorker, 09/30/2013)
Episode Credits
Guests:
- Hana Fields, outreach manager, Health Outreach Prevention Education
- Dr. Patrick Sullivan, professor of epidemiology, Emory University Rollins School of Public Health
- Brad Sullivan
- Jeremiah Johnson, executive director, PrEP4All
- Dr. John Brooks, former chief medical officer for the Centers for Disease Control and Prevention Division of HIV/AIDS Prevention
- Dr. Brett Giroir, former assistant secretary for health, U.S. Department of Health and Human Services
The Tradeoffs theme song was composed by Ty Citerman. Additional music this episode from Blue Dot Sessions and Epidemic Sound.
Additional thanks to Lindsey Dawson, Amy Killelea, Harold Phillips, Marcus Dillender, James Kublin and Valerie Howard.
This episode was produced by Melanie Evans, edited by Dan Gorenstein and mixed by Andrew Parrella.
You must be logged in to post a comment.